Dr David Bell, ME/CFS Specialist; NY, USA
Mitochondrial Dysfunction
JOURNAL HIGHLIGHTS, UNDERSTANDING CFS | 13. JUN, 2011 BY GUEST CONTRIBUTOR
Dr. David Bell
By David S. Bell, M.D., F.A.A.P.
Reprinted with permission from Lyndonville News, Vol. 8, Issue 1
This article is directed toward the mitochondrial problems which underlie the energy envelope of ME/CFS. [Editor's note: More info about the energy envelope.] Whatever is the cause of ME/CFS results in poor mitochondrial functioning and reduced energy output. Drs. Norman Booth, Sarah Myhill and John McLaren-Howard have been very kind as to write a clarification of the paper by Vermulen et al. discussed below and an update of their own work. I feel that it is at the cutting edge. First let’s put the energy production problems in perspective.
There has been talk for many years about the mitochondrial problems present in persons with CFS. In 1990 I did a muscle biopsy study looking for large insertions and the general morphology of mitochondria with Dr. June Aprille of Tufts University. Our results showed no mitochondrial DNA large (>240 bp) insertions and normal morphology, but this study was never published. Since then, my interests have continued around the mitochondria, particularly in the area of energy production. There have been nearly 30 scientific papers concerning oxidative stress, and many other papers concerning mitochondria in persons with CFS.
In a previous issue of Lyndonville News, I summarized the elegant study of Drs. Sarah Myhill, Norman Booth and John McLaren-Howard (Myhill S, Booth N, McLaren-Howard J. Chronic fatigue syndrome and mitochondrial dysfunction. International Journal of Clinical and Experimental Medicine. 2009;2:1-16).
More recent is this publication: Vermeulen R, Kurk R, Visser F, Sluiter W, Scholte H. Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. Journal of Translational Medicine 2010;8:93.
This paper is important in that it accomplishes two things: a) it confirms conference reports and abstracts about a decrease in anaerobic threshold on the second test of a test-retest protocol. b) it looks further at this phenomenon by determining that the decrease in ATP production is not due to a defect in the enzymes which carry out oxidative phosphorylation. There must be some other factor, as yet unknown, which causes this.
The authors tested 15 CFS women and 15 healthy sedentary control women with exercise tests separated by 24 hours (test-re-test). ATP synthesis rate was determined along with creatine kinase levels, used as a surrogate measure of lowered oxidative phosphorylation. The anaerobic threshold of patients was worse than sedentary controls on both first and second tests, with the second test showing a significant decline. However measures of CK and ATP synthesis rates based upon degree of reduction in complex I and II were not different from the two groups. The effort of patients and controls in the exercise was the same. Interestingly, pulmonary parameters indicated a possibility of a ventilation-perfusion mismatch in the patient group.
Drs. Norman Booth, John McLaren-Howard, and Sarah Myhill were kind to write the following commentary that is linked to the paper in Readers’ Comments:
Neutrophil ATP Related Parameters in Chronic Fatigue Syndrome
It is gratifying to see experts in the biomedical field turn their attention to the devastating illness Chronic Fatigue Syndrome (CFS/ME), as exemplified in the recent paper by Vermeulen et al [1]. Further studies of the postexertional malaise following exercise, either physical or mental, are extremely important because this malaise is the most characteristic and disabling symptom of CFS/ME. Moreover, in spite of many studies, there is inadequate understanding of the biochemical processes which lead to this malaise.
In 2009, we published our findings from an audit where we compared deficiencies in the provision of ATP in neutrophils with the degree of disability of patients with CFS/ME [2]. The results presented were from 53 controls and 71 CFS patients (61 in the same age range 18-65 years as the controls). The patient group spanned a wide range of CFS Ability from 0 to 7 on the Bell CFS Ability scale [2-3].
The paper by Vermeulen et al [1] compares exercise performance in CFS patients and controls. These authors conclude that the decrease in mitochondrial ATP production with work rate detected in their tests on peripheral blood mononuclear cells (PBMCs) is a secondary phenomenon. They focus attention on differences in transport capacity of oxygen. While agreeing about the importance of this and supporting the premise that more research is needed to understand oxygen transport-related issues in CFS, a number of ATP-related issues concern us greatly.
Vermeulen et al quote the excellent work by Maianski et al [4] on neutrophils in support of their dismissal of the importance of ATP-related parameters in CFS. The work in [4] concentrates on the aspects restricted to apoptosis. The work of van Raam et al [5] further defines these issues and shows that neutrophils retain some respiratory chain complex activity but this activity is limited to certain complexes in the respiratory chain and exists mainly for the maintenance of mitochondrial membrane potential.
These papers raise critical doubt about the validity of our previous findings and we feel that it is important to explore these issues in terms of the ATP-related tests we have done and the results we have published together with some preliminary comments comparing the CFS patients in the Vermeulen et al [1] study and our own [2].
With regard to the exercise procedures given to the 15 CFS patients in the Vermeulen et al study, we are confident that many of the patients in our study, including all of those in the ‘severe’ and ‘very severe’ categories would not have been able to carry out the exercise procedures. While we fully appreciate that the patients in both studies met the Centers for Disease Control criteria for CFS [6], we are well aware that there is enormous patient-to-patient variability in the degree of physical and mental incapacity. We felt it a strength of our paper that the measured biochemical parameters were compared individually and collectively with the CFS Ability [2-3] of the individual patients. This was, of course, much simpler with the higher number of patients in our study.
We now discuss the issues relating to neutrophil ATP-related parameters in the three parts of the ATP profile test that we used.
Whole cell ATP
ATP often functions as a complex with magnesium (Mg) and in many reactions Mg is an essential cofactor. Due to the fact that intracellular Mg deficiencies are common in CFS, we measured the whole cell ATP in neutrophils in the presence of excess Mg and again with endogenous Mg only.
The mean of the whole cell ATP level of our control group as measured with excess Mg was 2.00 ± 0.33 fmol/cell (SD, n=53). The distribution was highly asymmetric with a sharp cut-off at 1.6 and a tail extending up to 2.9 fmol/cell as illustrated in the right-hand histogram in Figure 2A of our paper [2]. The mean with endogenous Mg only was 1.37 ± 0.23 fmol/cell, with a distribution of almost identical shape to that of the whole cell ATP due to the fact that the ratio (defined as ATP Ratio and shown in Figure 2B our paper) has almost the same value 0.686 ± 0.032 for all the controls. The ATP concentrations given in Figure 1 of the Maianski et al paper [4] and confirmed in Figure 4 of van Raam et al [5] lie between our results with and without added Mg. These differences in baseline whole cell ATP may simply relate to differing Mg concentration or other methodological differences in the test procedures.
In our profile, we have used the ATP Ratio as an indication of the Mg status of the CFS patients. We found that about 70% of the patients were deficient in Mg as compared with the controls. Also, 87% were below the minimum value of the controls in the ATP with only endogenous Mg, ATPend as shown below in Fig 1. In spite of this, the value of ATPend was not a strong indicator of CFS Ability with a correlation coefficient of only r = 0.086. It is as if a low ATPend is a prerequisite for CFS but does not determine the severity of the illness. A more likely explanation is that the normal vigorous motility of the neutrophils is suppressed such that they are only just alive with about ½ of the ATPend of the controls.
JOURNAL HIGHLIGHTS, UNDERSTANDING CFS | 13. JUN, 2011 BY GUEST CONTRIBUTOR
Dr. David Bell
By David S. Bell, M.D., F.A.A.P.
Reprinted with permission from Lyndonville News, Vol. 8, Issue 1
This article is directed toward the mitochondrial problems which underlie the energy envelope of ME/CFS. [Editor's note: More info about the energy envelope.] Whatever is the cause of ME/CFS results in poor mitochondrial functioning and reduced energy output. Drs. Norman Booth, Sarah Myhill and John McLaren-Howard have been very kind as to write a clarification of the paper by Vermulen et al. discussed below and an update of their own work. I feel that it is at the cutting edge. First let’s put the energy production problems in perspective.
There has been talk for many years about the mitochondrial problems present in persons with CFS. In 1990 I did a muscle biopsy study looking for large insertions and the general morphology of mitochondria with Dr. June Aprille of Tufts University. Our results showed no mitochondrial DNA large (>240 bp) insertions and normal morphology, but this study was never published. Since then, my interests have continued around the mitochondria, particularly in the area of energy production. There have been nearly 30 scientific papers concerning oxidative stress, and many other papers concerning mitochondria in persons with CFS.
In a previous issue of Lyndonville News, I summarized the elegant study of Drs. Sarah Myhill, Norman Booth and John McLaren-Howard (Myhill S, Booth N, McLaren-Howard J. Chronic fatigue syndrome and mitochondrial dysfunction. International Journal of Clinical and Experimental Medicine. 2009;2:1-16).
More recent is this publication: Vermeulen R, Kurk R, Visser F, Sluiter W, Scholte H. Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. Journal of Translational Medicine 2010;8:93.
This paper is important in that it accomplishes two things: a) it confirms conference reports and abstracts about a decrease in anaerobic threshold on the second test of a test-retest protocol. b) it looks further at this phenomenon by determining that the decrease in ATP production is not due to a defect in the enzymes which carry out oxidative phosphorylation. There must be some other factor, as yet unknown, which causes this.
The authors tested 15 CFS women and 15 healthy sedentary control women with exercise tests separated by 24 hours (test-re-test). ATP synthesis rate was determined along with creatine kinase levels, used as a surrogate measure of lowered oxidative phosphorylation. The anaerobic threshold of patients was worse than sedentary controls on both first and second tests, with the second test showing a significant decline. However measures of CK and ATP synthesis rates based upon degree of reduction in complex I and II were not different from the two groups. The effort of patients and controls in the exercise was the same. Interestingly, pulmonary parameters indicated a possibility of a ventilation-perfusion mismatch in the patient group.
Drs. Norman Booth, John McLaren-Howard, and Sarah Myhill were kind to write the following commentary that is linked to the paper in Readers’ Comments:
Neutrophil ATP Related Parameters in Chronic Fatigue Syndrome
It is gratifying to see experts in the biomedical field turn their attention to the devastating illness Chronic Fatigue Syndrome (CFS/ME), as exemplified in the recent paper by Vermeulen et al [1]. Further studies of the postexertional malaise following exercise, either physical or mental, are extremely important because this malaise is the most characteristic and disabling symptom of CFS/ME. Moreover, in spite of many studies, there is inadequate understanding of the biochemical processes which lead to this malaise.
In 2009, we published our findings from an audit where we compared deficiencies in the provision of ATP in neutrophils with the degree of disability of patients with CFS/ME [2]. The results presented were from 53 controls and 71 CFS patients (61 in the same age range 18-65 years as the controls). The patient group spanned a wide range of CFS Ability from 0 to 7 on the Bell CFS Ability scale [2-3].
The paper by Vermeulen et al [1] compares exercise performance in CFS patients and controls. These authors conclude that the decrease in mitochondrial ATP production with work rate detected in their tests on peripheral blood mononuclear cells (PBMCs) is a secondary phenomenon. They focus attention on differences in transport capacity of oxygen. While agreeing about the importance of this and supporting the premise that more research is needed to understand oxygen transport-related issues in CFS, a number of ATP-related issues concern us greatly.
Vermeulen et al quote the excellent work by Maianski et al [4] on neutrophils in support of their dismissal of the importance of ATP-related parameters in CFS. The work in [4] concentrates on the aspects restricted to apoptosis. The work of van Raam et al [5] further defines these issues and shows that neutrophils retain some respiratory chain complex activity but this activity is limited to certain complexes in the respiratory chain and exists mainly for the maintenance of mitochondrial membrane potential.
These papers raise critical doubt about the validity of our previous findings and we feel that it is important to explore these issues in terms of the ATP-related tests we have done and the results we have published together with some preliminary comments comparing the CFS patients in the Vermeulen et al [1] study and our own [2].
With regard to the exercise procedures given to the 15 CFS patients in the Vermeulen et al study, we are confident that many of the patients in our study, including all of those in the ‘severe’ and ‘very severe’ categories would not have been able to carry out the exercise procedures. While we fully appreciate that the patients in both studies met the Centers for Disease Control criteria for CFS [6], we are well aware that there is enormous patient-to-patient variability in the degree of physical and mental incapacity. We felt it a strength of our paper that the measured biochemical parameters were compared individually and collectively with the CFS Ability [2-3] of the individual patients. This was, of course, much simpler with the higher number of patients in our study.
We now discuss the issues relating to neutrophil ATP-related parameters in the three parts of the ATP profile test that we used.
Whole cell ATP
ATP often functions as a complex with magnesium (Mg) and in many reactions Mg is an essential cofactor. Due to the fact that intracellular Mg deficiencies are common in CFS, we measured the whole cell ATP in neutrophils in the presence of excess Mg and again with endogenous Mg only.
The mean of the whole cell ATP level of our control group as measured with excess Mg was 2.00 ± 0.33 fmol/cell (SD, n=53). The distribution was highly asymmetric with a sharp cut-off at 1.6 and a tail extending up to 2.9 fmol/cell as illustrated in the right-hand histogram in Figure 2A of our paper [2]. The mean with endogenous Mg only was 1.37 ± 0.23 fmol/cell, with a distribution of almost identical shape to that of the whole cell ATP due to the fact that the ratio (defined as ATP Ratio and shown in Figure 2B our paper) has almost the same value 0.686 ± 0.032 for all the controls. The ATP concentrations given in Figure 1 of the Maianski et al paper [4] and confirmed in Figure 4 of van Raam et al [5] lie between our results with and without added Mg. These differences in baseline whole cell ATP may simply relate to differing Mg concentration or other methodological differences in the test procedures.
In our profile, we have used the ATP Ratio as an indication of the Mg status of the CFS patients. We found that about 70% of the patients were deficient in Mg as compared with the controls. Also, 87% were below the minimum value of the controls in the ATP with only endogenous Mg, ATPend as shown below in Fig 1. In spite of this, the value of ATPend was not a strong indicator of CFS Ability with a correlation coefficient of only r = 0.086. It is as if a low ATPend is a prerequisite for CFS but does not determine the severity of the illness. A more likely explanation is that the normal vigorous motility of the neutrophils is suppressed such that they are only just alive with about ½ of the ATPend of the controls.
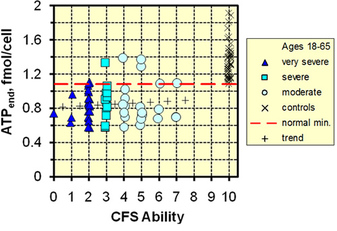
Fig 1. Plot of ATPend = ATP x (ATP Ratio) vs CFS Ability
We did not compare baseline whole cell ATP levels in neutrophils and PBMCs. It is clear from van Raam et al [5] that although their ATP levels are similar to ours, there are markedly differing effects of some known inhibitors of oxidative phosphorylation. As a result, Vermeulen et al [1] understandably criticize our use of neutrophils to explore ATP function in CFS patients. It is appropriate that we should proceed with further studies comparing neutrophils with PBMCs and we are doing so. Until such results are available, we wish to explain further aspects of the work already done and the tests we have used.
Inhibition study and ADP to ATP re-conversion
Following the measurement of the whole cell ATP, we used sodium azide to inhibit ATP production prior to a two-stage re-measurement of ATP. The azide ion is an inhibitor of cytochrome c oxidase, a component of Complex IV in the mitochondrial respiratory electron transfer chain. It is in the initial step that our results differ from those of Maianski et al [4]. Under the conditions in which we did the test, we saw a rapid (in less than 3 minutes) fall in measured ATP, usually to just a few percent (7.5 ± 3.4 % for the controls) of the starting value. After removal of the inhibitor, in our control group we saw the total ATP levels return to between 60% and 90% of their original values as shown in the right-hand histogram in Figure 2C of our paper [2]. Note also the strong negative feedback correlation between the degree of recovery and ATP concentration for the control group, shown in the upper right-hand corner of Figure 3B of our paper [2]. These results appear to be inconsistent with the findings shown in Figure 1 of Maianski et al [4]. However, they measured after 6 hours with and without inhibitor and also there may have been some compensatory process involved.
For the 38% of the patients who had similar recoveries to the controls, the degree of recovery was independent of CFS Ability, while for the other group (62% of the patients) with recoveries below 60% (and as low as less than 10%) there was a strong correlation with CFS Ability, as shown in Figure 2C of our paper [2] and in Fig 2 below. We attribute these low recovery values to an inability of the mitochondria to reliably reconvert ADP to ATP.
We did not compare baseline whole cell ATP levels in neutrophils and PBMCs. It is clear from van Raam et al [5] that although their ATP levels are similar to ours, there are markedly differing effects of some known inhibitors of oxidative phosphorylation. As a result, Vermeulen et al [1] understandably criticize our use of neutrophils to explore ATP function in CFS patients. It is appropriate that we should proceed with further studies comparing neutrophils with PBMCs and we are doing so. Until such results are available, we wish to explain further aspects of the work already done and the tests we have used.
Inhibition study and ADP to ATP re-conversion
Following the measurement of the whole cell ATP, we used sodium azide to inhibit ATP production prior to a two-stage re-measurement of ATP. The azide ion is an inhibitor of cytochrome c oxidase, a component of Complex IV in the mitochondrial respiratory electron transfer chain. It is in the initial step that our results differ from those of Maianski et al [4]. Under the conditions in which we did the test, we saw a rapid (in less than 3 minutes) fall in measured ATP, usually to just a few percent (7.5 ± 3.4 % for the controls) of the starting value. After removal of the inhibitor, in our control group we saw the total ATP levels return to between 60% and 90% of their original values as shown in the right-hand histogram in Figure 2C of our paper [2]. Note also the strong negative feedback correlation between the degree of recovery and ATP concentration for the control group, shown in the upper right-hand corner of Figure 3B of our paper [2]. These results appear to be inconsistent with the findings shown in Figure 1 of Maianski et al [4]. However, they measured after 6 hours with and without inhibitor and also there may have been some compensatory process involved.
For the 38% of the patients who had similar recoveries to the controls, the degree of recovery was independent of CFS Ability, while for the other group (62% of the patients) with recoveries below 60% (and as low as less than 10%) there was a strong correlation with CFS Ability, as shown in Figure 2C of our paper [2] and in Fig 2 below. We attribute these low recovery values to an inability of the mitochondria to reliably reconvert ADP to ATP.
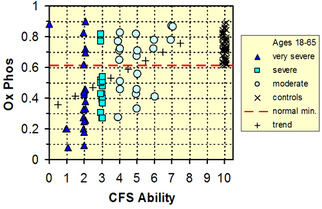
Fig 2. Plot of Ox Phos v Ability for patients and controls, age 18-65. The patients divide into 2 groups, one above and one below the normal minimum line. For the former group Ox Phos appears to be independent of CFS Ability while for the latter group there is a strong correlation with Ability. The trend line (+) averages over these 2 groups. In contrast, Vermeulen et al [1] conclude that mitochondrial ATP production shows no defect.
In order to make a comparison of the two studies we will have to ignore the fact that in our study the values of the Ox Phos parameter for the patients definitely fall into two groups, and we just take the average of all Ox Phos parameter values. However we do this for each value of CFS Ability. Also, for CFS Ability = 6 and 7 there are only 3 patients in each so we average the 6 patients and assign them CFS Ability = 6.5. Vermeulen et al [1] make 4 measurements of ATP synthesis (using methods developed to measure the activity of individual protein complexes in the mitochondrial electron transfer chain [5, 7]) and 1 of CK (creatine kinase) in plasma for CPET1 and CPET2 and for patients and for controls. The only convenient way to compare the two studies is to compare ratios of the mean value of each parameter for patients with the corresponding mean for the controls, <patients>/<controls>. Because we are just comparing mean values we can use the standard error of the mean (SEM) for each mean value rather than the larger standard deviation (SD). The results are shown in Fig 3.
In Fig 3A the Ox Phos ratios for the ‘moderate’ patients show only a slight decrease from unity while there is a strong decrease for the more severely ill patients. This shows that mitochondrial ADP-ATP recycling does occur in mitochondria of neutrophils and is strongly correlated with CFS illness severity. As mentioned previously, it is unlikely that any of the patients in the Vermeulen et al cohort were comparable with the ‘severe’ and ‘very severe’ patients so we show as red dotted lines the mean ± 1 SEM of the ‘moderate group. Average Ox Phos ratio of ‘moderate’ = 0.851 ± 0.065 (SEM, n=21).
In order to make a comparison of the two studies we will have to ignore the fact that in our study the values of the Ox Phos parameter for the patients definitely fall into two groups, and we just take the average of all Ox Phos parameter values. However we do this for each value of CFS Ability. Also, for CFS Ability = 6 and 7 there are only 3 patients in each so we average the 6 patients and assign them CFS Ability = 6.5. Vermeulen et al [1] make 4 measurements of ATP synthesis (using methods developed to measure the activity of individual protein complexes in the mitochondrial electron transfer chain [5, 7]) and 1 of CK (creatine kinase) in plasma for CPET1 and CPET2 and for patients and for controls. The only convenient way to compare the two studies is to compare ratios of the mean value of each parameter for patients with the corresponding mean for the controls, <patients>/<controls>. Because we are just comparing mean values we can use the standard error of the mean (SEM) for each mean value rather than the larger standard deviation (SD). The results are shown in Fig 3.
In Fig 3A the Ox Phos ratios for the ‘moderate’ patients show only a slight decrease from unity while there is a strong decrease for the more severely ill patients. This shows that mitochondrial ADP-ATP recycling does occur in mitochondria of neutrophils and is strongly correlated with CFS illness severity. As mentioned previously, it is unlikely that any of the patients in the Vermeulen et al cohort were comparable with the ‘severe’ and ‘very severe’ patients so we show as red dotted lines the mean ± 1 SEM of the ‘moderate group. Average Ox Phos ratio of ‘moderate’ = 0.851 ± 0.065 (SEM, n=21).
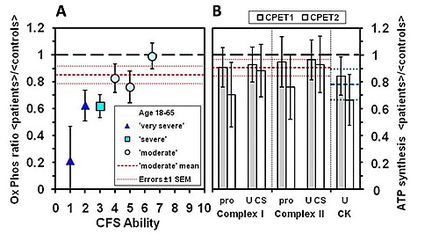
Fig 3. Comparison of A. Ox Phos data in neutrophils [2] with B. ATP synthesis data in PBMC and CK in plasma [1]. The labels pro and U CS refer to the ATP synthesis rate expressed as nmol/0.5 h. per mg protein or per U citrate synthase.
In Fig 3B the Complex I and II ratios are all less than unity but the errors are so large that they are also consistent with no decrease from unity. However, they are also consistent with the decreases of the ‘moderate’ group of patients. The red dotted lines indicate the average over all Complex I and II ATP synthesis values (± 1 SEM), and the blue dotted lines the average and ± 1 SEM of the CK values. Average ratio of ATP synthesis rates = 0.905 ± 0.062.
This number overlaps the Ox Phos number and we conclude that the ATP synthesis data cannot support the statement that mitochondrial ATP production shows no defect. The Ox Phos data show that decreased oxidative phosphorylation is not a major factor for ‘moderate’ patients, but becomes very important for the more severely disabled patients.
The third part of our ATP profile test explored the functionality of the translocator protein (TL or ANT for adenine nucleotide transporter), the electrogenic antiport which transports ADP into mitochondria for recycling. It also transports the ATP synthesized by recycling back into the cytosol where it is used.
ADP – ATP translocator (TL) study
Neutrophils contain fewer mitochondria than PBMCs but there are sufficient for study purposes. It is clear from van Raam et al [5] that we may not be studying the whole respiratory chain but rather the reconversion of ADP to ATP by some of the complexes. Indeed, this was what we wanted to study although we fully accept that the use of mitochondria from PBMCs rather than neutrophils may have proved a better option.
We separated mitochondria from neutrophils and made 3 aliquots of the separated mitochondria. The first was used to measure ATP within the mitochondria. The second aliquot was provided with excess ADP and the third aliquot deprived of ADP. The exact analysis conditions were decided experimentally and designed to maximize the production of mitochondrial ATP from ADP (parameter TL OUT), and the provision of ATP to the external artificial cytoplasm (parameter TL IN). In this way we explored the efficiency of ADP-ATP translocator (TL) sites in the mitochondrial inner membrane.
In our control group the baseline mitochondrial ATP increase was greater than 35% in the TL OUT part of the test with excess ADP present, while 60% of the CFS patients failed to exceed this minimum production of ATP. In the TL IN part of the test where access to ADP was restricted, the mitochondrial ATP decrease was between 50 and 75% for the control group. For 30/61 (or 50%) of the patients the decrease in the mitochondrial ATP was less than for the controls indicating a blocking of ATP transfer to the artificial cytosol. Both of these parameters show strong correlation with CFS Ability. The results are summarized in Fig 4 where we show the product (TL OUT) x (TL IN) as a function of CFS Ability. Note the strong correlation with r = 0.683.
One of us (JMH) has proceeded with further studies of TL function and has found chemical blocking in such cases. The results of molecular level fluorescence microscopy and the identification of the blocking agents by Micro Raman Spectroscopy and Fourier Transform Infrared Spectroscopy will be the subject of a further paper.
Conclusions
Our study [2] compared ATP-related parameters in CFS patients and in a similar number of controls. We have found that neutrophils are suitable for such a study and that they reflect the severity of CFS and can provide insight into appropriate therapeutic strategies.
In retrospect, we can see that this work using neutrophils should have been paralleled by similar studies using PBMCs and we have already begun that task. In the interim, we commend the results of our paper as a significant contribution to understanding the energy depletion in CFS patients. The laboratory findings closely paralleled the functional ability of the patients. This in no way belittles the contribution made by Vermeulen et al [1] who conclude that transport capacity of oxygen is limited in CFS patients. We wish to see both of these avenues of investigation explored more fully.
In Fig 3B the Complex I and II ratios are all less than unity but the errors are so large that they are also consistent with no decrease from unity. However, they are also consistent with the decreases of the ‘moderate’ group of patients. The red dotted lines indicate the average over all Complex I and II ATP synthesis values (± 1 SEM), and the blue dotted lines the average and ± 1 SEM of the CK values. Average ratio of ATP synthesis rates = 0.905 ± 0.062.
This number overlaps the Ox Phos number and we conclude that the ATP synthesis data cannot support the statement that mitochondrial ATP production shows no defect. The Ox Phos data show that decreased oxidative phosphorylation is not a major factor for ‘moderate’ patients, but becomes very important for the more severely disabled patients.
The third part of our ATP profile test explored the functionality of the translocator protein (TL or ANT for adenine nucleotide transporter), the electrogenic antiport which transports ADP into mitochondria for recycling. It also transports the ATP synthesized by recycling back into the cytosol where it is used.
ADP – ATP translocator (TL) study
Neutrophils contain fewer mitochondria than PBMCs but there are sufficient for study purposes. It is clear from van Raam et al [5] that we may not be studying the whole respiratory chain but rather the reconversion of ADP to ATP by some of the complexes. Indeed, this was what we wanted to study although we fully accept that the use of mitochondria from PBMCs rather than neutrophils may have proved a better option.
We separated mitochondria from neutrophils and made 3 aliquots of the separated mitochondria. The first was used to measure ATP within the mitochondria. The second aliquot was provided with excess ADP and the third aliquot deprived of ADP. The exact analysis conditions were decided experimentally and designed to maximize the production of mitochondrial ATP from ADP (parameter TL OUT), and the provision of ATP to the external artificial cytoplasm (parameter TL IN). In this way we explored the efficiency of ADP-ATP translocator (TL) sites in the mitochondrial inner membrane.
In our control group the baseline mitochondrial ATP increase was greater than 35% in the TL OUT part of the test with excess ADP present, while 60% of the CFS patients failed to exceed this minimum production of ATP. In the TL IN part of the test where access to ADP was restricted, the mitochondrial ATP decrease was between 50 and 75% for the control group. For 30/61 (or 50%) of the patients the decrease in the mitochondrial ATP was less than for the controls indicating a blocking of ATP transfer to the artificial cytosol. Both of these parameters show strong correlation with CFS Ability. The results are summarized in Fig 4 where we show the product (TL OUT) x (TL IN) as a function of CFS Ability. Note the strong correlation with r = 0.683.
One of us (JMH) has proceeded with further studies of TL function and has found chemical blocking in such cases. The results of molecular level fluorescence microscopy and the identification of the blocking agents by Micro Raman Spectroscopy and Fourier Transform Infrared Spectroscopy will be the subject of a further paper.
Conclusions
Our study [2] compared ATP-related parameters in CFS patients and in a similar number of controls. We have found that neutrophils are suitable for such a study and that they reflect the severity of CFS and can provide insight into appropriate therapeutic strategies.
In retrospect, we can see that this work using neutrophils should have been paralleled by similar studies using PBMCs and we have already begun that task. In the interim, we commend the results of our paper as a significant contribution to understanding the energy depletion in CFS patients. The laboratory findings closely paralleled the functional ability of the patients. This in no way belittles the contribution made by Vermeulen et al [1] who conclude that transport capacity of oxygen is limited in CFS patients. We wish to see both of these avenues of investigation explored more fully.
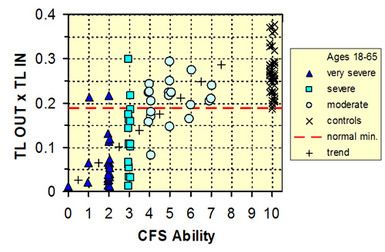
Fig 4. Plot of the product (TL OUT x (TL IN) as a function of CFS Ability.
References
1. Vermeulen R, Kurk R, Visser F, Sluiter W, Scholte H: Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. Journal of Translational Medicine 2010, 8:93.
2. Myhill S, Booth NE, McLaren-Howard J: Chronic fatigue syndrome and mitochondrial dysfunction. International Journal of Clinical and Experimental Medicine 2009, 2:1-16.
3. Bell DS: The Doctor’s Guide to Chronic Fatigue Syndrome. New York: Da Capo Press; 1994.
4. Maianski NA, Geissler J, Srinivasula SM, Alnemri ES, Roos D, Kuijpers TW: Functional characterization of mitochondria in neutrophils: a role restricted to apoptosis. Cell Death and Differentiation 2004, 11:143-153.
5. van Raam BJ, Sluiter W, de Wit E, Roos D, Verhoeven AJ, Kuijpers TW: Mitochondrial Membrane Potential in Human Neutrophils Is Maintained by Complex III Activity in the Absence of Supercomplex Organisation. PLoS ONE 2008, 3:e2013.
6. Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A: The chronic fatigue syndrome: a comprehensive approach to its definition and study. Annals of Internal Medicine 1994, 121:953-959.
7. Barrientos A: In vivo and in organello assessment of OXPHOS activities. Methods 2002, 26:307-316.
_______________
Dr. David Bell graduated from Harvard College in 1967 with an AB degree in English literature followed by Boston University with an MD degree in 1971. Post doctoral training in pediatrics was completed in 1976 with subspecialty training in Pediatric Behavior and Developmental Disorders. In 1978 he began work at the University of Rochester but soon began a private practice in the town of Lyndonville, New York.
In 1985 nearly 220 persons became ill with an illness subsequently called chronic fatigue syndrome in the communities surrounding Lyndonville, New York. This illness cluster began a study of the illness which continues today. Dr. Bell is the author or co-author of numerous scientific papers on CFS, and, in 2003 was named Chairman of the Advisory Committee for Chronic Fatigue Syndrome of the Department of Health and Human Services. Publications include A Disease of A Thousand Names (1988) and The Doctor’s Guide to Chronic Fatigue Syndrome (1990).
Dr. Bell has recently retried from general medicine and lives with his wife, Nancy, a family nurse practitioner, in Lyndonville. Roughly half of the patients seen in his former medical practice suffer from chronic fatigue syndrome, fibromyalgia, orthostatic intolerance, and/or myalgic encephalomyelitis. In addition to serving patients through his practice, Dr. Bell has been active in research and education of professionals and patients alike. He has served on many boards and panels, including the Board of Directors of the CFIDS Association of America from 1992-1997.
Share and Enjoy
References
1. Vermeulen R, Kurk R, Visser F, Sluiter W, Scholte H: Patients with chronic fatigue syndrome performed worse than controls in a controlled repeated exercise study despite a normal oxidative phosphorylation capacity. Journal of Translational Medicine 2010, 8:93.
2. Myhill S, Booth NE, McLaren-Howard J: Chronic fatigue syndrome and mitochondrial dysfunction. International Journal of Clinical and Experimental Medicine 2009, 2:1-16.
3. Bell DS: The Doctor’s Guide to Chronic Fatigue Syndrome. New York: Da Capo Press; 1994.
4. Maianski NA, Geissler J, Srinivasula SM, Alnemri ES, Roos D, Kuijpers TW: Functional characterization of mitochondria in neutrophils: a role restricted to apoptosis. Cell Death and Differentiation 2004, 11:143-153.
5. van Raam BJ, Sluiter W, de Wit E, Roos D, Verhoeven AJ, Kuijpers TW: Mitochondrial Membrane Potential in Human Neutrophils Is Maintained by Complex III Activity in the Absence of Supercomplex Organisation. PLoS ONE 2008, 3:e2013.
6. Fukuda K, Straus SE, Hickie I, Sharpe MC, Dobbins JG, Komaroff A: The chronic fatigue syndrome: a comprehensive approach to its definition and study. Annals of Internal Medicine 1994, 121:953-959.
7. Barrientos A: In vivo and in organello assessment of OXPHOS activities. Methods 2002, 26:307-316.
_______________
Dr. David Bell graduated from Harvard College in 1967 with an AB degree in English literature followed by Boston University with an MD degree in 1971. Post doctoral training in pediatrics was completed in 1976 with subspecialty training in Pediatric Behavior and Developmental Disorders. In 1978 he began work at the University of Rochester but soon began a private practice in the town of Lyndonville, New York.
In 1985 nearly 220 persons became ill with an illness subsequently called chronic fatigue syndrome in the communities surrounding Lyndonville, New York. This illness cluster began a study of the illness which continues today. Dr. Bell is the author or co-author of numerous scientific papers on CFS, and, in 2003 was named Chairman of the Advisory Committee for Chronic Fatigue Syndrome of the Department of Health and Human Services. Publications include A Disease of A Thousand Names (1988) and The Doctor’s Guide to Chronic Fatigue Syndrome (1990).
Dr. Bell has recently retried from general medicine and lives with his wife, Nancy, a family nurse practitioner, in Lyndonville. Roughly half of the patients seen in his former medical practice suffer from chronic fatigue syndrome, fibromyalgia, orthostatic intolerance, and/or myalgic encephalomyelitis. In addition to serving patients through his practice, Dr. Bell has been active in research and education of professionals and patients alike. He has served on many boards and panels, including the Board of Directors of the CFIDS Association of America from 1992-1997.
Share and Enjoy
 RSS Feed
RSS Feed
