I used dr. K. deMeirleir's Protea Biopharma Neurotoxic Metabolite Test Kit which aims to detect the presence of abnormal metabolites in the urine. It is a simple DIY kit that costs £25-35. These metabolites are related to the production of hydrogen sulphide (H2S), which is present in the body in small amounts under normal conditions and has certain physiological roles. An excess can be very detrimental, causing neurotoxic symptoms like photo-sensitivity, overload phenomenon and other symptoms of ME/CFS. Over-production of H2S is related to gut dysbiosis - too many bad bugs and not enough beneficial ones. DeMeirleir has concluded that a large proportion of people with ME/CFS present with such dysbiosis.
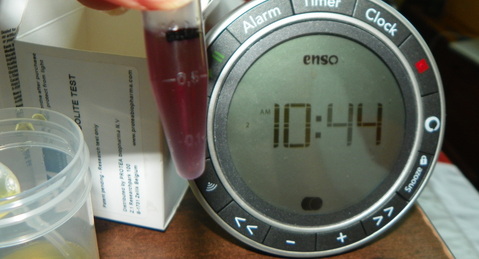
ME/CFS: H2S test. My sample turned violet right away; this shot is 15 seconds into the test.

ME/CFS: H2S test. My sample after the required 3-minute wait period, now opaque and deep violet.
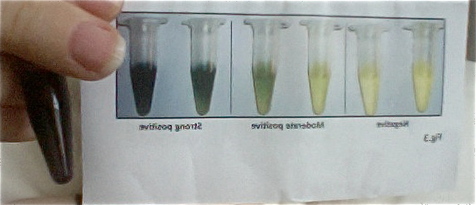
ME/CFS: H2S test. The reference range for the H2S test: the square on the right is negative; the square in the middle is mildly positive; the final, darkest square is a strong positive.

My sample demonstrates a strong positive for H2S. My Comprehensive Digestive and Stool Analysis showed no significant pathogens, though a high index of dysbiosis was present with 0% L. acidophilous (after 12 years of taking Natren, VSL#3, kefir and others), and low bifidus. I do not eat any sugars or grains.
My cousin with ME/CFS also took VSL#3 and kefir (among other things), yet seemed to find improvement in test results which translated to a great improvement in his ME/CFS.
My cousin with ME/CFS also took VSL#3 and kefir (among other things), yet seemed to find improvement in test results which translated to a great improvement in his ME/CFS.


 RSS Feed
RSS Feed
